A ring-shaped rash does not automatically mean ringworm — and applying antifungal cream to the wrong condition can delay recovery or make things worse. Five common skin conditions produce circular rashes that are routinely mistaken for ringworm, each requiring a completely different treatment approach.

Need Care Today?
Get a same-day telehealth visit with a board-certified provider.
Licensed in PA, MD, WA & DE
Book a Visit →Ringworm vs. Lookalike Rashes — Quick Reference
| Condition | Scaly? | Itchy? | Contagious? | Key Difference |
|---|---|---|---|---|
| Ringworm (tinea) | Yes | Yes | Yes | Raised scaly border, central clearing |
| Pityriasis Rosea | Mildly | Mildly | No | Herald patch first; spreads in Christmas tree pattern |
| Granuloma Annulare | No | Rarely | No | Smooth firm bumps, not flaky |
| Nummular Eczema | Yes | Very | No | Weeps/oozes; worse in winter |
| Lyme Rash (EM) | No | Rarely | No | After tick bite — needs antibiotics |
| Contact Dermatitis | No | Yes | No | Shape matches what touched skin (jewelry, bandage) |
How to Identify Ringworm
Ringworm, known medically as tinea corporis, is a fungal infection of the skin caused by dermatophytes -- not an actual worm. The hallmark appearance is a red, scaly, ring-shaped patch with raised borders and central clearing. As the fungus spreads outward from the center, the outer edge remains active and inflamed while the interior skin may look relatively normal, creating that distinctive ring pattern. The rash is usually itchy, and it tends to grow slowly over days to weeks if left untreated.
True ringworm is contagious and can be spread through direct skin-to-skin contact, shared towels or clothing, or contact with infected pets. It is more common in warm, humid environments and in areas of the body prone to sweating. The rash may appear anywhere on the trunk, arms, or legs, and when it affects the scalp, groin, or feet, it goes by different names such as tinea capitis, tinea cruris (jock itch), or tinea pedis (athlete's foot).
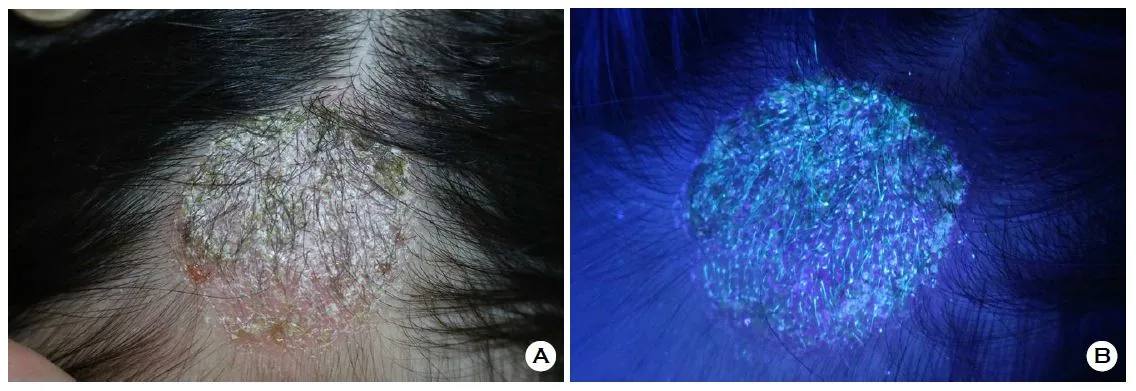
(A) Tinea capitis (scalp ringworm) under normal light showing a scaly, crusted patch. (B) The same lesion under Wood's lamp ultraviolet light revealing characteristic blue-green fluorescence from the Microsporum fungus. Source: Choi J, et al. Journal of Mycology and Infection (Open Access, CC BY-NC).
A provider can often diagnose ringworm based on its appearance alone, but additional diagnostic tools can confirm the diagnosis. A Wood's lamp (ultraviolet light) examination can cause certain dermatophyte species to fluoresce a characteristic blue-green color, though not all ringworm species produce fluorescence. Dermoscopy -- using a handheld magnifying device with polarized light -- allows clinicians to examine the rash at higher magnification, revealing patterns in the scale, hair follicles, and vascular structures that differ between fungal infections and their mimics. In some cases, a skin scraping examined under a microscope with potassium hydroxide (KOH prep) or a fungal culture may be needed for definitive confirmation. This step is particularly important because several other skin conditions produce circular or ring-shaped rashes that closely resemble ringworm -- and each one requires a different treatment approach. Applying antifungal cream to a rash that is not actually fungal can delay proper care and sometimes make the condition worse.
Pityriasis Rosea: The Most Common Ringworm Lookalike

Pityriasis rosea: oval scaly patches on the torso. Unlike ringworm, pityriasis rosea starts with a single herald patch and spreads in a Christmas tree pattern.
Pityriasis rosea is one of the most frequently misidentified conditions in dermatology because it often begins with a single oval or round patch that looks strikingly similar to ringworm. This initial lesion, called a "herald patch," typically appears on the chest, back, or abdomen and measures two to four centimeters across. It has a slightly raised, scaly border with pinkish or salmon-colored skin in the center -- a pattern that is easy to confuse with a fungal ring.
Within one to two weeks of the herald patch, a secondary eruption of smaller oval patches spreads across the torso. These patches tend to follow the natural creases of the skin, creating what clinicians sometimes describe as a "Christmas tree" pattern on the back. Unlike ringworm, which usually remains as one or a few isolated rings, pityriasis rosea involves dozens of patches appearing in a short time frame. Mild itching is common, but many patients notice only the cosmetic changes.
The exact cause of pityriasis rosea is not fully understood, though it is thought to be related to a reactivation of certain human herpesvirus strains (HHV-6 or HHV-7). The condition is not contagious and typically resolves on its own within six to eight weeks without treatment. If itching is bothersome, a provider may recommend antihistamines, gentle moisturizers, or a short course of low-potency topical corticosteroids. Recognizing this pattern early can save you from unnecessary antifungal treatments. If you have a rash you are unsure about, a telehealth visit can help clarify the diagnosis.
Granuloma Annulare vs Ringworm

Granuloma annulare: smooth, firm, ring-shaped bumps that mimic ringworm. Unlike ringworm, the surface is not scaly or flaky, and the condition is not contagious. Image: Wikimedia Commons (CC BY-SA).
Granuloma annulare is a benign inflammatory skin condition that forms smooth, firm, ring-shaped bumps under the skin. The rings are typically skin-colored, reddish, or slightly violaceous and range from one to five centimeters in diameter. Because of the circular shape, it is frequently mistaken for ringworm -- but there are important differences. Granuloma annulare lacks the flaky, scaly texture that characterizes a fungal infection. The surface of the ring is smooth rather than rough, and the center may appear slightly sunken or normal rather than clearing with visible scale.
This condition most commonly appears on the hands, feet, elbows, and knees, though it can develop anywhere. It tends to affect children and young adults more often than older individuals, and it is not contagious or caused by infection. The exact cause remains unclear, but it is believed to involve a localized immune reaction in the deeper layers of the skin. In most cases, granuloma annulare is completely asymptomatic -- patients notice the ring but do not experience itching or pain.
Most cases of granuloma annulare resolve spontaneously within one to two years without any treatment, though recurrence is common. For persistent or widespread cases, a provider may consider topical corticosteroids, cryotherapy, or other targeted therapies. If you have a ring-shaped bump that does not respond to over-the-counter antifungal cream after two weeks of consistent use, granuloma annulare should be considered as an alternative diagnosis.
Nummular Eczema: Another Ring-Shaped Rash
Nummular eczema, also called nummular dermatitis or discoid eczema, produces coin-shaped patches of irritated skin that are easily confused with ringworm. The word "nummular" comes from the Latin word for coin, reflecting the round or oval shape of these lesions. Unlike ringworm, nummular eczema patches are typically uniformly inflamed throughout rather than showing central clearing. They tend to be very itchy, crusted, and may weep or ooze clear fluid, especially in the acute phase.
This form of eczema is more common in middle-aged and older adults, particularly during dry winter months when the skin barrier is compromised. It often appears on the legs, arms, and torso. Contributing factors include very dry skin, frequent hot showers, harsh soaps, and environmental irritants. People with a personal or family history of atopic dermatitis, asthma, or allergies are at higher risk. Unlike ringworm, nummular eczema is not infectious and cannot be passed from person to person.
Treatment focuses on restoring the skin barrier and reducing inflammation. This typically includes frequent application of thick emollient moisturizers, avoidance of known triggers, and prescription-strength topical corticosteroids or calcineurin inhibitors for active flares. Antifungal treatments are ineffective against nummular eczema and may actually irritate the skin further. If you have round, itchy patches that are not improving with antifungal cream, it is worth discussing nummular eczema with a provider.
Lyme Disease Rash vs Ringworm

Erythema migrans: the classic bullseye rash of Lyme disease. Note the concentric red rings with central clearing — this pattern is distinct from ringworm's scaly border. Source: CDC Public Health Image Library (public domain).
The erythema migrans rash of early Lyme disease is one of the most important ringworm lookalikes to recognize because it signals an active bacterial infection that requires prompt antibiotic treatment. This rash develops at the site of a tick bite, typically three to thirty days after exposure, and expands gradually over several days. It often forms a large red circle or oval that can reach ten centimeters or more in diameter -- much larger than a typical ringworm lesion. In some cases, it develops a characteristic "bull's-eye" or target-like pattern with a central red area, a pale ring, and an outer red ring.
There are several key differences between erythema migrans and ringworm. The Lyme disease rash is usually flat and smooth rather than scaly or raised. It expands more rapidly than ringworm, sometimes growing noticeably over just a day or two. It is often warm to the touch but may not be particularly itchy. Systemic symptoms such as fatigue, body aches, fever, and headache frequently accompany the rash, which is uncommon with a simple fungal infection. The rash also tends to appear in areas where ticks attach, such as the groin, armpit, waistline, or behind the knee.
If you develop an expanding circular rash after spending time outdoors in an area where ticks are present -- particularly in the mid-Atlantic, Northeast, or upper Midwest regions of the United States -- seek medical evaluation promptly. Early Lyme disease is highly treatable with a course of oral antibiotics such as doxycycline, but delayed treatment can lead to joint, neurological, and cardiac complications. A telehealth provider can assess the rash through photos and video, order appropriate testing, and start treatment the same day if Lyme disease is suspected.
Contact Dermatitis That Mimics Ringworm
Contact dermatitis occurs when the skin reacts to a substance it touches, producing redness, swelling, and sometimes blistering. When the offending substance contacts the skin in a circular or arc-shaped pattern -- such as from a round bandage, a watchband, a nickel button, or a circular patch of adhesive -- the resulting rash can look remarkably like ringworm. Allergic contact dermatitis from jewelry is one of the most common scenarios, where a ring or bracelet leaves a red, itchy, circular mark on the skin.
There are two main types of contact dermatitis: irritant and allergic. Irritant contact dermatitis results from direct chemical damage to the skin and can happen to anyone given enough exposure. Allergic contact dermatitis is a delayed immune reaction that develops after repeated exposure to a specific allergen. Common culprits include nickel in jewelry, fragrances in lotions and detergents, latex, adhesives, and certain preservatives in skincare products. The shape of the rash corresponds directly to the area of contact rather than spreading outward like a fungal infection.
The treatment for contact dermatitis centers on identifying and avoiding the trigger substance. Cool compresses, gentle fragrance-free moisturizers, and topical corticosteroids can help manage symptoms during a flare. If a circular rash appears in a location that coincides with where jewelry, clothing, or a product touches your skin, contact dermatitis is a strong possibility. A telehealth rash evaluation can help you determine the cause and develop a plan to prevent future reactions.
When to See a Provider for a Circular Rash
While many circular rashes are harmless and self-limiting, certain features warrant prompt medical evaluation. You should see a provider if your rash is expanding rapidly over the course of days, if it is accompanied by fever or body aches, if it appeared after a known or possible tick bite, or if it involves blistering, open sores, or significant pain rather than just itching. A rash that does not improve after two weeks of over-the-counter antifungal treatment is another clear signal that something other than ringworm may be at play.
It is also important to seek care if you have multiple ring-shaped lesions appearing simultaneously, if the rash is located on the face or near the eyes, or if you have a weakened immune system due to medications or a medical condition. In immunocompromised patients, both fungal infections and their lookalikes can present atypically, making professional evaluation especially valuable.
Many circular rashes can be accurately assessed through telehealth. Clear, well-lit photographs of the rash combined with a detailed history -- including when it appeared, how it has changed, whether you have been exposed to new products or environments, and any associated symptoms -- give a provider the information needed to distinguish between ringworm and its many mimics. From there, a targeted treatment plan can be started right away, saving you the frustration of trial-and-error with the wrong medications.
Frequently Asked Questions
How can I tell if my circular rash is ringworm?
Ringworm typically presents as a red, scaly ring with clearing in the center that gradually expands. It is usually itchy and may appear on the arms, legs, or torso. A provider can often distinguish ringworm from lookalike conditions based on appearance, location, and history.
What is pityriasis rosea?
Pityriasis rosea is a common, harmless skin condition that starts with a single large oval patch called a herald patch, followed by smaller oval patches on the torso. It often resolves on its own within 6 to 8 weeks.
Can a telehealth provider diagnose a rash?
Yes. Many rashes can be evaluated via telehealth using photos and video. A provider can assess your rash, discuss symptoms, and recommend treatment or refer you for further evaluation if needed.
When should I worry about a circular rash?
Seek medical attention if a circular rash is expanding rapidly, is painful rather than itchy, has blisters or open sores, appears after a tick bite, or does not improve after two weeks of treatment.
What common conditions have a ring-shaped rash that looks like ringworm?
Five conditions are commonly mistaken for ringworm: pityriasis rosea (harmless, resolves in 6–8 weeks), granuloma annulare (smooth bumps, not scaly), nummular eczema (coin-shaped, very itchy), Lyme disease rash or erythema migrans (after a tick bite — requires antibiotics), and contact dermatitis (reaction where something touched the skin). Each requires a different treatment, which is why an accurate diagnosis matters.
Should I use OTC antifungal cream on any ring-shaped rash?
No. Over-the-counter antifungal creams like clotrimazole or terbinafine only help true fungal infections. Using them on eczema, granuloma annulare, or pityriasis rosea will not help and can sometimes cause irritant dermatitis. If a rash does not improve within 1 to 2 weeks of treatment, get it evaluated rather than continuing to guess.
What does the Lyme disease rash look like?
The classic Lyme rash (erythema migrans) is a slowly expanding red patch that often grows larger than 5 cm over several days, sometimes with central clearing that gives it a bull's-eye look. It usually starts 3 to 30 days after a tick bite and may come with fever, headache, fatigue, or joint pain. If you have this rash, it needs prompt antibiotic treatment.
Can stress trigger a ring-shaped rash?
Stress does not cause ringworm, but it can flare conditions like nummular eczema or contact dermatitis that produce similar shapes. Improving sleep, reducing irritant exposure, and using gentle skin care can help. If a rash is persistent, very itchy, or spreading, an evaluation is still worthwhile.
How quickly should ringworm respond to antifungal treatment?
Most cases of true ringworm on the body improve noticeably within 1 to 2 weeks of consistent topical antifungal use, with full treatment lasting 2 to 4 weeks. Scalp ringworm and nail fungus require oral antifungal therapy and longer treatment. If your rash is unchanged or worse after 2 weeks of correct use, it is probably not ringworm.
Can InnoCre diagnose and treat rashes by photo and video in MD, WA, or DE?
Yes. InnoCre evaluates rashes by photo and video for adults and adolescents 12 and older in Maryland, Washington, or Delaware. We can prescribe non-controlled treatments like topical antifungals, topical steroids, or antibiotics when indicated, and refer you to a local dermatologist for in-person workup if a rash needs a biopsy or is not improving.
What's the difference between herald patch vs ringworm?
When evaluating herald patch vs ringworm, clinicians consider viral infection, skin rashes, pityriasis rosea vs ringworm, and affected areas. An InnoCre telehealth visit covers a same-day symptom review, lab orders at a local lab when needed, and a prescription sent to your pharmacy if appropriate.
How does an InnoCre telehealth visit work?
After you book, you complete a short intake form, then connect with a board-certified provider by video on the same day in most cases. The provider reviews your symptoms and history, orders lab work at a local lab if needed, and sends any prescription to the pharmacy of your choice. A new-patient visit is a flat $68 with no insurance required.
Get the Care You Need Today
A board-certified provider can evaluate your symptoms and recommend treatment. Same-day visits available for patients in Pennsylvania, Maryland, Washington, and Delaware.
Book a Visit →Visits start at $68 · HSA/FSA accepted · PA, MD, WA & DE
Atul S. Vellappally, DNP, CRNP, FNP-BC
Founder, InnoCre Telehealth. Board-certified Family Nurse Practitioner with doctoral-level training in evidence-based and precision medicine. Licensed in Pennsylvania, Maryland, Washington, and Delaware.
This article is for informational purposes only and does not constitute medical advice. If you are experiencing a medical emergency, call 911.
Related Services
Related Articles
Sources
Clinical references used in this article:
- Ringworm Basics. Centers for Disease Control and Prevention.
- Clinical Overview of Ringworm. Centers for Disease Control and Prevention.
- About Fungal Diseases. Centers for Disease Control and Prevention.
- Rashes. MedlinePlus, National Library of Medicine.